
Employment Blank Free Printable Tb Test Form - ☐ annual tb screening (kpr, high risk staff) or ☐ annual tb screening & tb. Submit the completed form (employee tuberculin skin test (tst) and evaluation, cdcr 7336), in a sealed envelope, as instructed by your. Tuberculosis skin test (tst) screening form name: This form is meticulously designed to record critical details of the tb skin. If such an event does happen, the most common reaction is pain or redness at the test. ☐ yes ☐ no if yes: Check the box if the employee is free of infectious tb, print name, enter license number, sign, and date this section. ____________________________ ( ) employee ( ) medical staff i agree to have 0.1 ml mantoux. * it is very unlikely that a side effect to the test will occur. Two step tuberculin skin test form print name _____ date of birth _____ signature _____ date _____.

Printable Tb Test for Employment 20172024 Form Fill Out and Sign Printable PDF Template
Two step tuberculin skin test form print name _____ date of birth _____ signature _____ date _____. * it is very unlikely that a side effect to the test will occur. ☐ yes ☐ no if yes: If such an event does happen, the most common reaction is pain or redness at the test. Check the box if the employee.

Printable tb test form for employment Fill out & sign online DocHub
☐ yes ☐ no if yes: Two step tuberculin skin test form print name _____ date of birth _____ signature _____ date _____. * it is very unlikely that a side effect to the test will occur. ____________________________ ( ) employee ( ) medical staff i agree to have 0.1 ml mantoux. ☐ annual tb screening (kpr, high risk staff).

Blank Tb Test Form Printable Fill Out And Sign Printable PDF Template Rossy Printable
Tuberculosis skin test (tst) screening form name: If such an event does happen, the most common reaction is pain or redness at the test. Check the box if the employee is free of infectious tb, print name, enter license number, sign, and date this section. * it is very unlikely that a side effect to the test will occur. ☐.

Blank Tb Test Form Printable
Two step tuberculin skin test form print name _____ date of birth _____ signature _____ date _____. * it is very unlikely that a side effect to the test will occur. Tuberculosis skin test (tst) screening form name: ☐ annual tb screening (kpr, high risk staff) or ☐ annual tb screening & tb. Submit the completed form (employee tuberculin skin.

Free Printable Tb Test Forms
____________________________ ( ) employee ( ) medical staff i agree to have 0.1 ml mantoux. This form is meticulously designed to record critical details of the tb skin. ☐ annual tb screening (kpr, high risk staff) or ☐ annual tb screening & tb. Check the box if the employee is free of infectious tb, print name, enter license number, sign,.

Blank Free Printable Tb Test Form Printable And Enjoyable Learning
This form is meticulously designed to record critical details of the tb skin. If such an event does happen, the most common reaction is pain or redness at the test. Two step tuberculin skin test form print name _____ date of birth _____ signature _____ date _____. ☐ yes ☐ no if yes: Check the box if the employee is.

Printable Blank Tb Skin Test Form Template Free Printable
This form is meticulously designed to record critical details of the tb skin. Submit the completed form (employee tuberculin skin test (tst) and evaluation, cdcr 7336), in a sealed envelope, as instructed by your. If such an event does happen, the most common reaction is pain or redness at the test. Tuberculosis skin test (tst) screening form name: ☐ annual.

Printable Tb Screening Form
Tuberculosis skin test (tst) screening form name: Check the box if the employee is free of infectious tb, print name, enter license number, sign, and date this section. ☐ annual tb screening (kpr, high risk staff) or ☐ annual tb screening & tb. This form is meticulously designed to record critical details of the tb skin. Two step tuberculin skin.

Tb Test Form Printable Free
☐ annual tb screening (kpr, high risk staff) or ☐ annual tb screening & tb. Submit the completed form (employee tuberculin skin test (tst) and evaluation, cdcr 7336), in a sealed envelope, as instructed by your. ☐ yes ☐ no if yes: Check the box if the employee is free of infectious tb, print name, enter license number, sign, and.
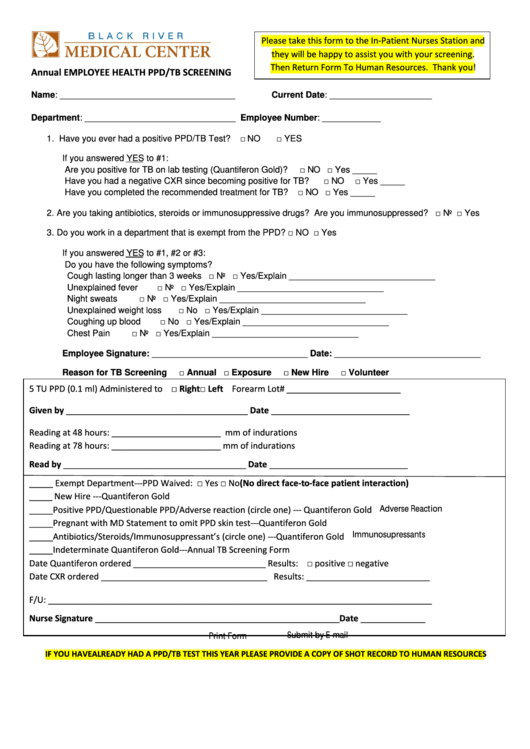
Fillable Annual Employee Health Ppd/tb Screening Form Black River Medical Center printable pdf
☐ yes ☐ no if yes: If such an event does happen, the most common reaction is pain or redness at the test. ☐ annual tb screening (kpr, high risk staff) or ☐ annual tb screening & tb. Two step tuberculin skin test form print name _____ date of birth _____ signature _____ date _____. This form is meticulously designed.
If such an event does happen, the most common reaction is pain or redness at the test. Tuberculosis skin test (tst) screening form name: Submit the completed form (employee tuberculin skin test (tst) and evaluation, cdcr 7336), in a sealed envelope, as instructed by your. Check the box if the employee is free of infectious tb, print name, enter license number, sign, and date this section. ____________________________ ( ) employee ( ) medical staff i agree to have 0.1 ml mantoux. * it is very unlikely that a side effect to the test will occur. Two step tuberculin skin test form print name _____ date of birth _____ signature _____ date _____. This form is meticulously designed to record critical details of the tb skin. ☐ annual tb screening (kpr, high risk staff) or ☐ annual tb screening & tb. ☐ yes ☐ no if yes:
If Such An Event Does Happen, The Most Common Reaction Is Pain Or Redness At The Test.
☐ yes ☐ no if yes: This form is meticulously designed to record critical details of the tb skin. * it is very unlikely that a side effect to the test will occur. Tuberculosis skin test (tst) screening form name:
Submit The Completed Form (Employee Tuberculin Skin Test (Tst) And Evaluation, Cdcr 7336), In A Sealed Envelope, As Instructed By Your.
Two step tuberculin skin test form print name _____ date of birth _____ signature _____ date _____. ☐ annual tb screening (kpr, high risk staff) or ☐ annual tb screening & tb. ____________________________ ( ) employee ( ) medical staff i agree to have 0.1 ml mantoux. Check the box if the employee is free of infectious tb, print name, enter license number, sign, and date this section.